
Dr. Dunaief is Assistant Professor of Ophthalmology, and Dr. Charkoudian is a resident, F.M. Kirby Center for Molecular Ophthalmology, Scheie Eye Institute, University of Pennsylvania, Philadelphia, PA.
If you are past your mid-fifties and you are having vision problems, you may be worried about developing age-related macular degeneration, or AMD. AMD is the leading cause of adult visual impairment and blindness in the world's developed nations. While there is no surefire way to prevent or to cure this disease, medical science has made great strides in understanding who gets the disease and why, as well as developing several promising new treatments.
Signs and Symptoms
As its name implies, the disease causes a gradual loss of function in the part of the eye called the macula. Located near the center of the retina, the macula plays a key role in sharply focused and central, as opposed to peripheral, vision. When AMD causes the macula to degenerate, the result is blurring or darkness at the center of a person's field of vision. While the degeneration usually takes years, there may be a sudden change in vision over a period of days. It also causes loss of the fine vision needed for reading, driving and recognizing other people's faces. To those in the later stages of AMD, printed words may appear blurry and straight lines may appear wavy. Peripheral vision usually remains unaffected by AMD and the disease almost never causes total blindness. Other classic signs of the disease are the development of drusen, or small spots on the eye, and color changes in the macula (see Figure 1 on next page).
Advanced AMD takes two forms: "wet" AMD, in which many small blood vessels grow into the cornea, leak and destroy photoreceptors, a phenomenon known technically as neovascularization; and "dry" AMD, which causes the loss of photoreceptors by a different process.To those in the later stages of AMD, printed words may appear blurry and straight lines may appear wavy. Peripheral vision usually remains unaffected by AMD...
Who Gets AMD and Why
Right now, an estimated 7 million individuals in the U.S. have intermediate AMD and 1.75 million have advanced AMD. Although 80% of these have the non-neovascular, or "dry," form, the neovascular, or "wet," form is responsible for most cases of severe visual loss. As its name implies, age-related macular degeneration becomes more common with age and is very rare in people younger than 55. For some reason, advanced AMD is significantly more prevalent in white people than among African-Americans or Hispanics.
The exact cause of AMD is not clear, but — like many age-related diseases — it most probably results from a combination of oxidative damage to bodily tissues, cardiovascular disease and genetic predisposition.
Oxidation
Oxidation occurs when oxygen molecules interact with other substances, including human tissue. Oxidation can be destructive, as when it causes iron to rust. Its exact effects depend on the amount of oxygen present and the nature of the material it touches. True oxidation happens on a molecular level. Within our bodies, for example, oxidation and so-called oxidative stress can damage certain cells and contribute to various diseases, including AMD.
We know that oxidation is associated with drusen formation. Research showing that antioxidants — certain vitamins and minerals taken in through our diet or in the form of nutritional supplements that combat oxidation — slow the progression of AMD further supports this idea. The presence of drusen is thought to lead to inflammation and a condition called oxidative stress. Oxidative damage accumulates over time, which is consistent with the age-related nature of the disease, as well as the gradual increase in number and size of drusen that characterizes AMD. Oxidative stress seems also to stimulate neovascularization.
Cardiovascular diseases such as hypertension and atherosclerotic (characterized by the buildup of plaque in the arteries) heart disease, are associated with an increased likelihood of developing AMD. Epidemiological surveys have also found higher rates of disease within families and among twins than in the general population, which suggests that there is a genetic aspect to the disease.
Research has also found evidence of a connection between AMD and overactivity of the immune system, which is known to cause inflammation and cellular damage.
Risk Factors
The main risk factors for AMD are:
Age
Large epidemiologic studies show that AMD becomes more common with age. The prevalence of AMD in individuals aged 75-85 years is more than three times that of individuals aged 43 to 54 years.
Ethnicity
Advanced disease is significantly more prevalent in white than in African-American or Hispanic populations. It may also be higher among Asians.
Smoking
Heavy smoking can double a person's risk for AMD. Stopping smoking reduces the odds of AMD reaching the advanced stage.
Genetic Factors
These have been shown to significantly increase the risk of disease.
Hypertension
Hypertension may be associated with increased risk of AMD, but the scientific evidence is conflicting.
Atherosclerotic Disease
Atherosclerotic cardiovascular disease may also be associated with increased risk of AMD but the data are conflicting.
Other risk factors include poor diet — i.e., low intake of antioxidant-rich foods and high intake of saturated fats and cholesterol — and, possibly, excessive exposure to sunlight.
Prevention
There is no proven way of preventing AMD. It stands to reason, however, that raising dietary intake of antioxidants and avoiding cigarette smoking would help. Taking antioxidant vitamin supplements has been shown in studies to lower the risk of progression from mild to advanced disease, but has not been proven to prevent the disease in the first place. Routine eye exams, of course, are recommended by national organizations and can screen for the disease. Regular eye examinations every 2-4 years are recommended for people aged 40-64 years and every 1-2 years for persons aged 65 years or older.
If you suspect you have some vision loss, you should see an ophthalmologist as soon as possible. Taking supplements with certain antioxidants (vitamin C 500 mg; vitamin E 400 IU; beta carotene 15 mg (25,000 IU); zinc oxide 80 mg; cupric oxide 2 mg) has been shown to slow the progression from intermediate AMD to advanced AMD. These micronutrients are recommended for anyone with intermediate AMD or anyone with advanced AMD in one eye. You can find products that combine these micronutrients into twice-daily supplements.
Smokers or recent ex-smokers are advised to take an antioxidant supplement without beta-carotene because taking high doses of beta-carotene may in fact increase the risk of lung cancer.35,36
How AMD Is Diagnosed
A routine eye examination by an ophthalmologist is typically sufficient to diagnose AMD. Further tests may be necessary to determine the severity of the disease and to determine treatment.
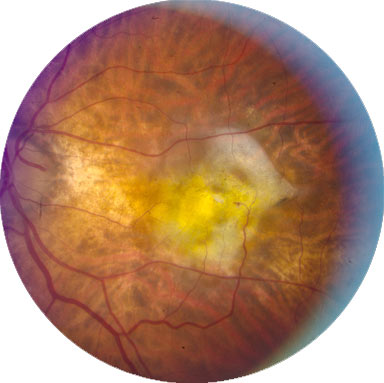
In the early stages of AMD, people often have no visual complaints or only very mild distortion. Those with the neovascular form of the disease often report a suddenly occurring distortion in the central visual field of one eye. Figures 1 to 3 below show early, intermediate and advanced examples of the disease, though advanced forms of AMD may be of subtypes (such as subretinal hemorrhage or retinal detachments) different from the one pictured here.
Figure 1.
Early Age-Related Macular Degeneration (AREDS Category 2).
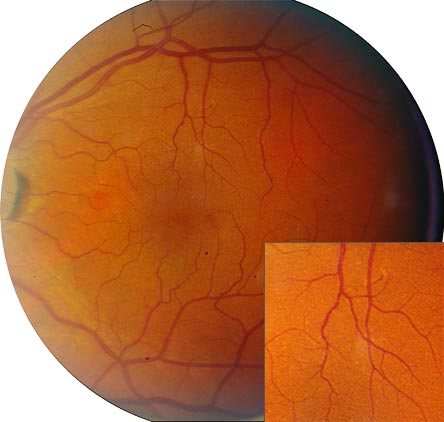
Figure 2.
Intermediate Age-Related Macular Degeneration (AREDS Category 3).
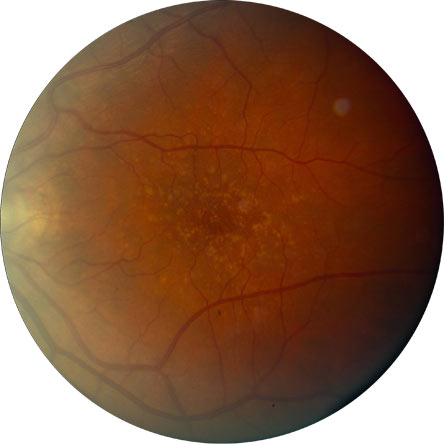
Figure 3.
Advanced AMD (AREDS Category 4) with a Subfoveal Fibrous Scar Resulting from Choroidal Neovascularization.
Imaging is also used to diagnose AMD. The most common types are:
Table 1.
Common Diagnostic Imaging Methods.
| Imaging Modality | Description |
|---|---|
| Fluorescein angiography | A vegetable-based dye is given intravenously and photographs are taken of the dye as it circulates in the retina. Leakage from neovascularization shows up as areas of expanding hyperfluorescence. |
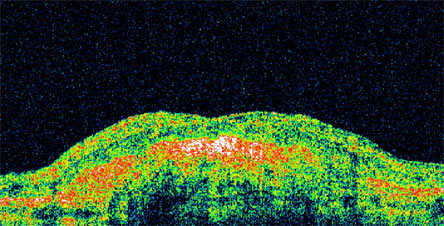
| Optical coherence tomography | A cross-section of the retina is obtained. The presence of intra-retinal or sub-retinal fluid may indicate neovascularization. Long-standing disease may show up as a dense scar. (see Figure 4) |
Figure 4.
Optical Coherence Tomography Image Showing a Dense Hyperreflective Scar.
Treatments Available for AMD
Treatments for ongoing, or active, neovascularization include:
Thermal Laser Photocoagulation
- Direct laser treatment of the area of neovascularization.
- May be preferred for certain types of neovascularization.
- Treatment is given as soon as possible after identification of active neovascularization to prevent irreversible retina damage. Treatment response is monitored with fluorescein angiography. Multiple treatments may be nlecessary.
Photodynamic Therapy
- Involves intravenous injection of a photosensitizer (a chemical compound that is excited by a specific light wavelength) and the application of a beam of light at the area of neovascularization.
- May be used for specific types of neovascularization.Considered next-best to VEGF inhibiting drugs as a therapy for active neovascularization. Currently used on an experimental basis in combination with VEGF inhibitors. Multiple treatments may be necessary.
- Patients are instructed to avoid sunlight and cover all exposed skin when outside for the first five days following therapy to avoid activation of the photosensitizer within the skin athat causes a burn-like reaction.
- Treatment of neovascularization by photodynamic therapy reduces the rate of vision loss, but most people will continue to experience a decline in vision.
Intravitreal VEGF Inhibitors
- Direct injection into the eye of a vascular endothelial growth factor-inhibiting drug (VEGF).
- VEGF inhibiting drugs include pegaptanib, ranibizumab and bevacizumab. Studies have shown ranibizumab and bevacizumab to be more effective than pegaptanib.
- Treatment is given as soon as possible after identification of neovascularization activity to prevent further damage. Effects are relatively short-lived. Typically, VEGF treatment is given as a series of injections (often monthly). Treatment response is monitored closely with optical coherence tomography and fluorescein angiography.
- This treatment carries a small risk of infection, retinal detachment or lens injury. Patients need to be aware of signs of eye infection (pain, decreased vision, significant light sensitivity and eye redness) and retinal detachment (new floaters, flashing lights and obscured visual field).
- Treatment of neovascularization by VEGF inhibiting drugs (i.e., ranibizumab or bevacizumab) improves vision in up to a third of patients and stabilizes vision in up to 95% of patients.
Summary
Advanced AMD, the category of AMD that causes the most extensive vision loss, has two forms: dry and wet. While no treatment is available for the dry form, vitamin supplements with high doses of the antioxidants lutein and zeaxanthin have been demonstrated by the National Eye Institute to slow the progression of dry macular degeneration and even to improve vision. Lutein and zeaxanthin are found naturally in foods such as kale, romaine lettuce, broccoli, zucchini, corn, spinach and Brussels sprouts.
The wet form of advanced AMD causes vision loss because of neovascularization, or abnormal blood vessel growth. Bleeding, leaking, and scarring from these blood vessels cause irreversible damage to the eye's photoreceptors and permanent vision loss.While no treatment is available for the dry form, vitamin supplements with high doses of the antioxidants lutein and zeaxanthin have been demonstrated...to slow the progression of dry macular degeneration...
Until recently, there have been no effective treatments for wet AMD. However, a new class of drugs called VEGF inhibitors is showing promise. When injected directly into the vitreous humor of the eye using a small needle, (while this sounds ghastly, there is no pain), these drugs can eliminate abnormal blood vessels and improve vision.
Certain types of neovascularization respond to Thermal Laser Photocoagulation and Photodynamic Therapy.
While there is no proof that diet can prevent AMD in the first place, the Age-Related Eye Disease Study (AREDS) showed that a combination of antioxiodants including beta-carotene, vitamin C, vitamin E, and zinc can lower the risk of developing advanced AMD by about 25 percent for people with the intermediate form of the disease.
As we have said, while there is no proven cause of AMD, the disease is associated with risk factors such as a high-fat, high-calorie diet; smoking and cardiovascular disease. Therefore, anyone who has reason to worry about developing AMD — e.g., because they have some risk factors or because it runs in the family — should consider addressing as many of these risk factors as possible. They should also talk with their physician about whether or not they should be taking antioxidant supplements and, above all, schedule regular eye examinations.
Resources
- Foundation for Fighting Blindness: Macular Degeneration - http://www.blindness.org/MacularDegeneration/
- MedlinePlus: Macular Degeneration - http://www.nlm.nih.gov/medlineplus/maculardegeneration.html
- National Eye Institute: Macular Degeneration - http://www.nei.nih.gov/health/maculardegen/armd_facts.asp
Guidelines
Age-Related Macular Preferred Practice Pattern. American Academy of Ophthalmology. 09/2006. http://www.aao.org/education/guidelines/ppp/amd_new.cfm - Non-algorithmic summary of the diagnosis and treatment of AMD.




