
Dr. Pignolo is Assistant Professor and Director, Ralston-Penn Clinic for Osteoporosis & Related Bone Disorders, Department of Medicine, Division of Geriatric Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA.
Though many people may not be familiar with it, Paget’s disease of bone (osteitis deformans) as it is formally known, it is the second most common bone disease after osteoporosis. The disease is a disorder of bone metabolism in which the bone remodels itself (breaks down and rebuilds) too quickly. This results in a bony overgrowth at various points as well as problems with the bone’s architecture.
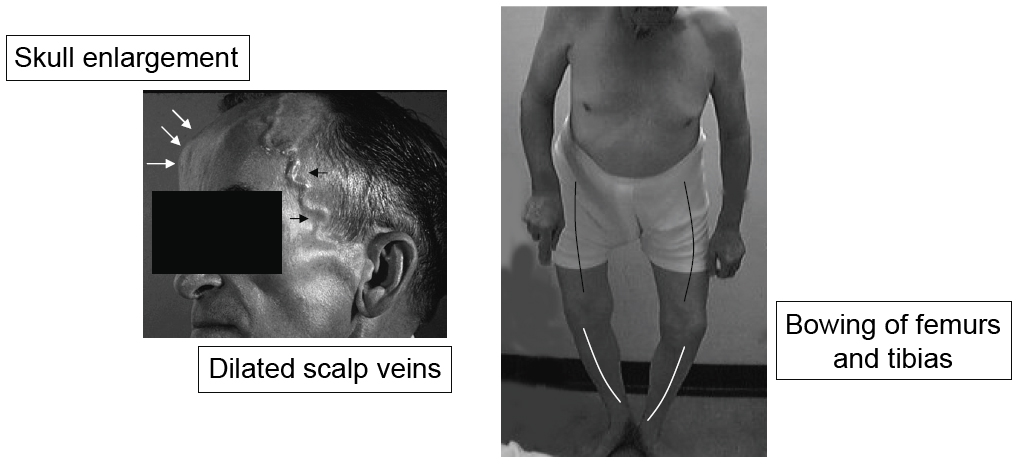
Patients who do have symptoms may complain of pain and have skeletal deformities that occur due to the overgrowth of affected bone.
First described in 1877 by Sir James Paget, Paget’s disease occurs when too much bone is reabsorbed and, as a result, excessive bone is rebuilt in undesirable ways. Sometimes patients have no symptoms, and in these cases, diagnosis may be made by chance, for example when a doctor orders x-rays for another reason. Other times, it can be diagnosed by identifying an enzyme in the blood called bone serum alkaline phosphatase. Patients who do have symptoms may complain of pain and have skeletal deformities that occur due to the overgrowth of affected bone. This feature will explain how Paget’s disease occurs, and how it is diagnosed and treated.
Like many other diseases, Paget's is likely the result of a combination of genetic and environmental factors. Up to one-quarter of family members of patients with Paget’s disease eventually contract the disease, with first-degree relatives having seven to ten times greater odds of developing the condition. Several genes have been identified in families with the disease
Viral infection may also play a role in who develops Paget’s disease. Osteoclasts — bone cells that eat up other bone cells for the purpose of "cleaning house" so that new bone can be laid down — from patients with Paget’s disease appear to contain viral particles, which are not found in osteoclasts from healthy individuals. In a small number of patients with Paget’s disease, certain bone and blood cells had virus particles that suggested the measles virus may be at play. Although a relationship between Paget’s disease and the canine distemper virus has been suggested in the owners of unvaccinated dogs, this possibility is controversial..
Osteoclasts — bone cells that eat up other bone cells for the purpose of "cleaning house" so that new bone can be laid down — from patients with Paget’s disease appear to contain viral particles.
When one looks at the bones of Paget’s disease patients under the microscope, they appear "disorganized" because so much bone has been reabsorbed and then replaced at an accelerated rate. There are several other changes that occur, one of which is that the collagen pattern is "immature", compared to the bones of healthy individuals.
Most patients are asymptomatic — they have no visible symptoms -- at the time they are diagnosed. As mentioned earlier, Paget’s disease is often discovered by blood work or by findings on an x-ray obtained for other reasons.
In patients who do show symptoms, pain and deformities of the skeleton usually point to the disease. In more advanced cases, fractures, tumors of the bone, neurologic issues, cardiac disease and calcium or phosphate imbalances may be present.
Paget’s disease may originally involve either a single bone (monostotic) or a few bones (polyostotic) but the process does not spontaneously spread to adjacent bones. In patients who do show symptoms, pain and deformities of the skeleton usually point to the disease. In more advanced cases, fractures, tumors of the bone, neurologic issues, cardiac disease and calcium or phosphate imbalances may be present. Less commonly, unexplained or excessive bleeding during orthopedic surgery may be the first signs of Paget’s disease.
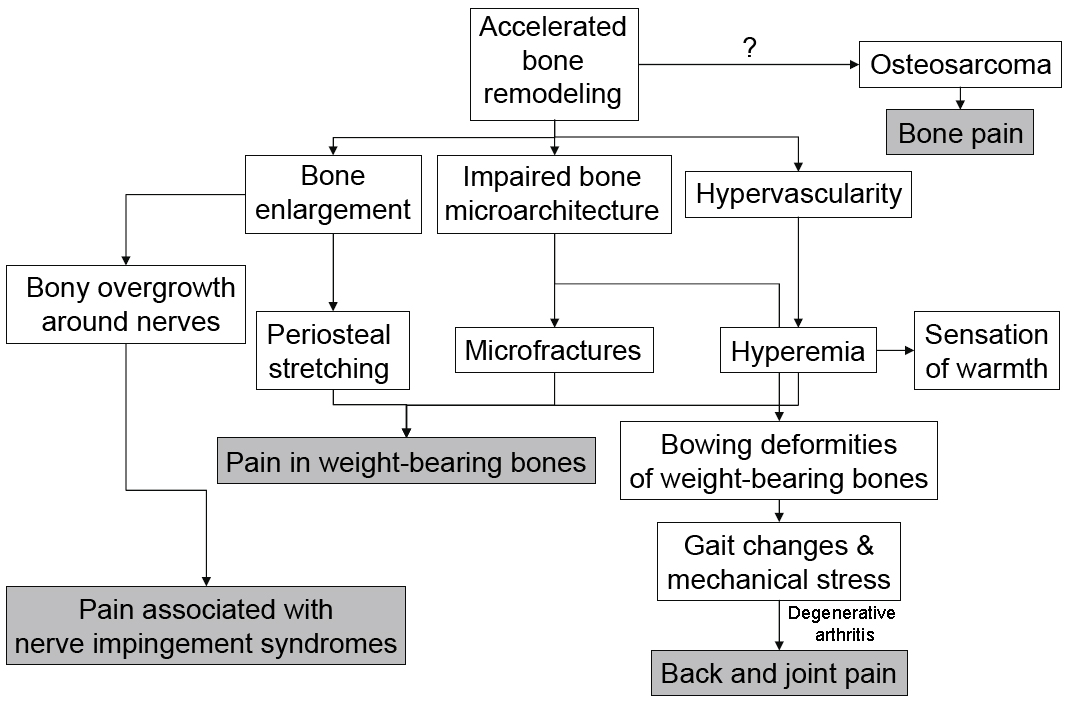
Signs and symptoms of Paget’s can vary quite a bit, and the variability relates to the location and the severity of the first sites of active disease in the skeleton. The most common places for these bone lesions to occur are the pelvis, spine, skull and long bones. Pain may occur at the particular site or in areas where complications arise secondary to degenerative arthritis, nerve impingement syndromes or osteosarcoma. Patients may feel pain through the course of their days, or it may be present at rest or get worse when resting or when the person is bearing weight, though these symptoms are nonspecific. It is quite possible to damage the joints that are adjacent to the bone deformities, and osteoarthritis (also causing pain) can also occur in the knees and hips. Figure 1 shows possible mechanisms for pain at active pagetic lesions or due to complications.
A doctor can identify Paget’s disease by plain radiographs (x-rays). There are a number of signs a clinician will look for, including areas where the bone has expanded or thickened. Many of these features can be viewed at http://www.paget.org.uk/info/tests.htm#xray.
Unfortunately, spontaneous fractures can occur in people with Paget’s disease, and may be either complete (if the bone is completely broken) or incomplete. Although some fractures can heal quickly, poor healing is a concern in the femur (thigh bone) bone.
After one’s doctor takes a careful history and performs a complete physical examination, he or she will measure the patient’s blood levels of alkaline phosphatase and calcium. A high level of alkaline phosphatase should raise suspicion for Paget’s disease in an otherwise healthy older patient.
A sensitive test for identifying bone lesions in Paget’s disease is for the doctor to identify "hot" spots using a bone scan which enables them to visualize the skeleton using injected radioactively-labeled chemicals.
A sensitive test for identifying bone lesions in Paget’s disease is for the doctor to identify "hot" spots using a bone scan which enables them to visualize the skeleton using injected radioactively-labeled chemicals. Plain radiographs (x-rays) can give additional information on neighboring joints, bone deformities, and other issues that might occur.
It is important for the doctor to distinguish on bone scans lesions resulting from Paget’s disease and those from metastatic bone disease — if this is not possible, further tests should be considered. If one’s doctor suspects malignancy, a CT scan, MRI or bone biopsy may also be done.
As mentioned earlier, many patients with Paget’s disease do not show symptoms, and therefore, they are not treated. Although some asymptomatic patients may benefit from treatment, the primary reasons for giving medication are to relieve symptoms (for example, pain and feelings of warmth) and to treat or prevent complications that come along with the disease. Asymptomatic patients with the involvement of weight-bearing long bones (i.e., the femur, pelvis), skull or spine should be treated so that deformities and other complications may be avoided.
The most effective treatments for Paget’s disease include non-pharmacological therapy, various pharmacological therapies (using either bisphosphonates or calcitonins) pain management and surgery
The symptoms that should get better with treatment are bone aches and pain, headache, , hypercalcemia and some symptoms of nerve compression. Unfortunately, bowing of the bones will not change with treatment. Deafness is also unlikely to improve. Pain from arthritis that develops as a result of the disease may or may not improve, but when both Paget’s disease and osteoarthritis are present, the arthritis may be treated first with acetaminophen or a nonsteroidal antiinflammatory drug (for example, ibuprofen).
Prophylactic (preventative) treatments may also be used in patients before surgery on the affected bone(s) to reduce the hypervascularity (increased number of blood vessels) that may result in excessive blood loss.
The most effective treatments for Paget’s disease include non-pharmacological therapy (i.e., physical therapy to improve muscle strength and mobility, and to control pain), various pharmacological therapies (using either bisphosphonates or calcitonins) pain management and surgery. Shoe inserts, orthotics — appliances which help stabilize body parts -- and devices to help patients walk, in addition to physical therapy, may be useful in addressing problems with one’s gait or other difficulties that result from bowing of the legs. Counseling patients on fall prevention and fractures (including care to avoid heavy lifting, sudden or strenuous twisting, turning or other types of movements depending on the location of the lesion), as well as weight control in overweight patients to put less pressure on one’s bones) may be helpful.
The drugs used to treat Paget's disease suppress the activity of the osteoclasts (the cells mentioned above that "eat" other bone cells). Bisphosphonates (such as the drugs prescribed for osteoporosis) and calcitonin are often used. Both have some side effects. For example, the side effects of calcitonin, may include nausea (10%), irritation at injection site (10%), flushed ears and face (10-20%), as well as some other rarer effects. Some people (about 50%) may develop calcitonin resistance when they are treated for more than six months. Bisphosphonates and other drugs carry other side effects.
Patients may also opt for elective surgeries such as joint replacement or repair of non-displaced fractures, which may help control pain symptoms. Corrective bone surgery for deformities that result from Paget’s disease is usually considered in cases where patients have problems with motion, pain, or with appearance, due to the deformed bone. Although hip replacement in Paget’s disease poses some challenges, they are performed in cases of gross deformities and under some other conditions.
In situations where Paget’s disease is particularly extensive, higher doses or more frequent dosing intervals of medications (i.e, a bisphosphate) may be required. Resistance to a specific compound may also develop, but use of an alternative drug may overcome this problem.
The Paget’s Association was founded in 1973 by Anne Stansfield MBE, who was driven by a lack of understanding and interest in the treatment of her husband who had Paget’s disease (http://www.paget.org.uk/). The Paget Foundation was founded in 1978 as a national voluntary health agency located in New York, NY, to provide information on Paget's disease of bone to patients, family members and health professionals (http://www.paget.org/).




