
Figure 1.
Cancer Death Rates* Among Women, by Cancer Site -- United States, 1930-1991.
*Rates are adjusted to the 1970 census population.
Source: American Cancer Society.
*Rates are adjusted to the 1970 census population.
Source: American Cancer Society.

Even before the first Surgeon General's report on smoking related illnesses (1964) was released, the number of male smokers in the U.S. was already decreasing. In the mid 1950s, close to 55% of the male population smoked; by 1993 it was 32%. On the other hand, in the mid 1950s, 25% of women smoked. The incidence actually increased to 35% in the early 1960s and then started a slow downturn, eventually paralleling males in the early 1980s (Fig. 2).
Figure 2.
Percentage of Adults Age = or >18 Years Who Are Current Cigarette Smokers,* by Sex -- United States, 1955-1993.
*Estimates since 1992 incorporate some-day smoking.
Source: Current Population Survey, 1995; National Health Interview Surveys, 1965-1993.
*Estimates since 1992 incorporate some-day smoking.
Source: Current Population Survey, 1995; National Health Interview Surveys, 1965-1993.

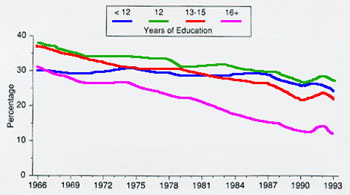
There are a few hopeful signs among young people. As opposed to the trend in the 1930s, college-bound young people are less likely to smoke. It is also true that the smoking incidence is lower in adults with the most years of formal education (Fig. 3).
Figure 3.
Percentage of Women Age = or >25 Years Who Are Current Cigarette Smokers,* by Education -- United States, 1965-1993.
*Estimates since 1992 incorporate some-day smoking.
Source: National Health Interview Surveys, 1965-1993
*Estimates since 1992 incorporate some-day smoking.
Source: National Health Interview Surveys, 1965-1993

Another trend is a sharp decrease in smoking by young African-American women (Fig. 4.
Figure 4.
Percentage of Female High School Seniors Who Are Daily Smokers,* by Race -- United States, 1976-1992.
*Smoking one or more cigarettes per day during the previous 30 days. Estimates are based on two-year floating averages.
Source: Institute for Social Research, University of Michigan, Monitoring the Future Project.
*Smoking one or more cigarettes per day during the previous 30 days. Estimates are based on two-year floating averages.
Source: Institute for Social Research, University of Michigan, Monitoring the Future Project.
Do Women and Men Smokers Differ?
More than men, women tend to medicate depression with smoking, use cigarettes to control their weight and their anger. However, this is not to say that men don't use cigarettes for these reasons as well.
Smoking and Depression
Smoking is more common in men and women with major depression and depression is twice as common in women. It is believed that nicotine is the main drug producing the mood elevating effect, but there may be others in tobacco smoke with similar effects. It is not surprising that the latest therapy for smoking cessation is an antidepressant medicine, burproprion.
Smoking and Anger
Women use smoking to control anger. Despite all the years of feminism, expression of anger by women remains socially unacceptable. Smoking is private and controllable and gives the appearance of relieving stress. Yet, it is possible that smoking, itself, may maintain stress for an established smoker is in a constant state of nicotine withdrawal, which can only be relieved by smoking.
Smoking and Weight Control
Ever since the advertising genius Edward Bernays thought up the motto, "Reach for a Lucky instead of a Sweet," tobacco advertising has strongly emphasized the pro-metabolic effects of nicotine. A 10% increase in metabolic rate occurs in a moderate smoker and, unless allowances are made for that at the time of cessation, weight gain will occur. More women are "supergainers" (25 lbs or more) than men.3 If you try to quit, you need to be prepared for the inevitable weight gain. Have low calorie snacks, like carrot and celery sticks, always available. A graded exercise program can be started. Women over 40 should have a cardiac stress test, particularly if they have other (in addition to smoking) coronary heart disease risk factors (i.e., family history, high blood pressure, high cholesterol or diabetes). "Weight" is not necessarily equated with fat. Weight gain from an exercise program may be from muscle -- more metabolically active than fat -- which will raise your metabolic rate.
How to Quit Smoking
Most smokers want to quit. Or, perhaps more accurately, they will say they wish they didn't smoke. Most regret they ever started. It is upsetting for people to find out that the youthful boast, "I can quit anytime," simply isn't true. Nicotine is addictive. The psychological habit of reaching for a cigarette at times of tension, stress, anger, or depression is powerful. The use of the cigarette as a social crutch, or as a signal to concentrate on a task, is a hard habit to break. That is why it takes three or four (or more) strong efforts to quit before long-term success is achieved.
There are now four types of Nicotine Replacement Therapy (NRT) and one antidepressant approved for smoking cessation. These treatments have different characteristics that can translate into specific advantages for individual smokers.
Several of the drugs are available over the counter (OTC). Though you can buy these drugs and use them on your own, I advise you to find (if possible) a helpful and sympathetic doctor who can counsel you and prescribe treatment if you need it to help you. Smoking is not a sin or a moral weakness. It is an addiction, a chronic disease that needs treatment before it kills you or spoils you life with a lot of illnesses. Enlist your doctor's help. Show the doctor this article and advise him/her to read the professional version. Help your doctor help a lot of people like you.
The cigarette habit isn't just about tobacco and inhaling smoke. It consists of dozens of unconsidered impulses which are reinforced hundreds or even thousands of times a day with every puff you take. Let's be honest. Nicotine is a wonderful drug. It calms you down and peps you up at the same time. What else does that? You will need preventive strategies to keep from smoking. You need to understand the urge, figure out why you liked smoking, recognize the "danger situations" and find substitute actions to take at those moments when the urge becomes nearly irresistible.
First, "clock" your habit. Write down every cigarette you smoke during the day and how important it was to smoke it. You need to know which are those "necessary" cigarettes, when the urge to smoke is the strongest. Then you think of other things you could do instead of smoking. Remember, the urge to smoke will go away whether you smoke or not. Identify "triggers," those situations or activities that are strongly associated with smoking. Finishing a meal, getting into your car, getting out of the subway station, picking up the telephone or going to a bar with friends, are some examples. Think of ways to avoid these trigger situation or an alternative activity or another "hand activity" to take the place of smoking.Every smoker is unique. That is why you have to look at your own situation and work out solutions. There is one problem that is very common -- alcohol.
Every smoker is unique. That is why you have to look at your own situation and work out solutions. There is one problem that is very common -- alcohol. If you want to quit smoking, alcohol is your Health Enemy Number One. Hang out with teetotalers (and non-smokers) and stay out of bars, especially in those first few months of quitting. Most people can't have JUST ONE. You are physically and pyschologically addicted.
Why am I telling you all this? Because the problem with the smoking habit is that it is not just nicotine. It is a ritual, a habit, a reflex. It has to be unlearned. You need to build up alternative habits and reflexes, which, as time goes on, become automatic and unconsidered, just like smoking was. It takes about three weeks to break a habit and three months of successful abstinence to strengthen these new habits to the point where relapse into smoking again is less likely.
Nicotine Replacement Therapy — NRT
For some people nicotine withdrawal is so uncomfortable they just cannot get through it. Withdrawal produces many symptoms. You can feel out of sorts, depressed, irritable, angry or unable to concentrate. Some people get so obnoxious that their friends, relatives or co-workers buy them cigarettes to calm them down again. You need to tell people around you that you are trying to quit and ask for their forbearance and help. Former smokers are particularly helpful. They've been there. Get yourself a buddy--someone to call for help and encouragement and to let off steam.
NRT eases nicotine withdrawal WHILE you are working on getting through urges, avoiding triggers and building up alternative ways of dealing with stress, tension, anger, etc.
Nicotine Replacement Therapy — Making It Work
Who is most likely to succeed with NRT? A daily smoker of 10 or more cigarettes per day. This type of smoker has a constant baseline blood level of nicotine. When nicotine is removed, the body has to adjust to a milieu with no nicotine. While that is happening, withdrawal symptoms occur. Intermittent, light or occasional smokers do not tend to have a baseline blood nicotine level, so medication aimed at easing physical nicotine withdrawal is unlikely to be effective.
With all forms of NRT, smoking must cease completely when using the NRT. Setting a quit date is key. You have to QUIT. This helps you do it. There must be absolutely no smoking when taking any form of nicotine replacement therapy. Some people who have cheated have experienced a severe sudden rise of their blood pressure and heart attacks.
Using the Different Forms of NRT
The Nicotine Patch...for those who need an automatic delivery system.
There are four kinds available:
- Nicoderm® 21mg, 14mg, 7mg, 24 hr patch — OTC
- Nicotrol® 15mg, 16 hr patch — OTC
- Habitrol® 21mg, 14mg, 7mg, 24 hr patch — prescription
- ProStep® 22mg, 11mg, 24 hr patch — prescription
The nicotine patch contains a nicotine compound that is absorbed into the body through the skin. It is applied in the morning and removed the following morning or before bedtime.
Some quitters complain of vivid dreams while wearing the patch at night. So removing it at bedtime is recommended, even with the so-called 24-hour patch. The other side effect is skin rash at the site of application. Moving the patch to a different area every day of the week may solve this problem.
Most patch-users are pleased with the effect of the patch. Many tell me that they applied it and simply forgot about it and also forgot to smoke. "If I'd known it would be so easy, I would have done it years ago," is a common comment.
Some patch types come in three strengths (Nicoderm® and Habitrol®). Smoking a pack or more a day requires the top strength. Stay on that one as long as you need it (say, six weeks) to be thoroughly out of the habit. Then work out a taper schedule. Don't get cocky. Take your time. It usually takes about three months. The Nicotrol® patch is meant to be used 16 hrs and taken off at bedtime. It is now recommended for six weeks. Six weeks without smoking is very good, but remember you are not "home free," especially during the first three months. You can use other NRT products or lower strength patches to keep you on track.
The Nicotine Gum — Nicorette® — OTC...For those who need oral stimulation
Nicorette® gum was the first type of NRT to be introduced. A nicotine compound is present in the surface of the gum. The nicotine is absorbed into the body through the membranes lining the mouth. It is poorly absorbed through the stomach. Therefore, it is very important to chew the gum correctly. The gum is initially chewed lightly until you sense a "peppery" taste. Then it is "parked" between the jaw below or above the teeth and the side of the cheek. Lightly chewing and parking are alternated for about 1/2 hour to get the full effect. There are currently two strengths of gum available- -2 mg and 4 mg. A heavy smoker (more than a pack per day) will find the 4 mg strength more helpful initially. Moderate smokers (1/2 - 1 pack per day) may do fine with 2 mg. The gum should be taken every 30 to 60 minutes at the beginning. Acid inactivates the nicotine compound, so rinsing the mouth with water after orange juice or coffee must be done before chewing a piece of gum. As mentioned before, chewing should not be vigorous, just intermittent, alternating with "parking" the gum. If chewing is vigorous, and the nicotine compound is swallowed, you may experience light-headedness, abdominal discomfort, hiccups and/or heartburn. These symptoms mean incorrect chewing technique. Read the directions and try again.
Chewing the gum at regular intervals results in a low steady level of nicotine in the blood. I find the gum particularly useful for people who are worried about weight gain because the gum occupies the mouth with a calorie-free substance. The gum is also useful for episodic smokers, who just need something to help them get over the urge.
Nicotine Nasal Spray - Nicotrol NS® - OTC...For those with sudden urges
This type of NRT reaches the brain the fastest. It is particularly helpful for those who are having a lot of trouble with urges. The nicotine compound is transferred into the blood stream through the membranes of the nose and the back of the throat. The starting dose is a spray into each nostril once or twice every hour. The dose is not to be sniffed or breathed in. You will be very uncomfortable if you inhale the medicine into your sinuses. Clear out your nasal passages, hold the inhaler to your nostril, don't breathe, tilt back your head and simply spray. Nasal congestion from a cold or allergy will make this treatment less effective. The main side effect is nasal irritation, which tends to decrease with continued use.
The Nicotine Inhaler - Nicotrol® Inhaler - prescription...For those who miss handling cigarettes.
The nicotine compound is in a small capsule, which is punctured and placed in a plastic mouthpiece that resembles a cigarette holder. Inhaling through the holder brings the aerosolized nicotine in contact with the back of the throat, where it is absorbed into the bloodstream. The effect is about the same as the gum. The nicotine compound really does not go down into the lungs. This form of NRT is particularly useful for smokers who find the habit of handling the cigarette important. The side effects are similar to the nasal spray -- throat irritation that lessens with use.
Summary of NRT
Each form of NRT has certain characteristic that might be helpful to individual smokers:
- the patch: automatic pilot
- the gum: mouth is busy, no calories
- the nasal spray: a quick hit for an urge
- the inhaler: something to handle
Can these forms of NRT be used in combination? Yes. You could wear the patch and add any of the other three to help with your particular problem:
- a piece of gum to keep from reaching for a piece of candy
- a nasal spray to get over an urge
- an inhaler to keep your hands busy
A Few Cautions Regarding NRT
Combinations will add to your nicotine level slightly, but remember, it would be very difficult to reach nicotine blood levels equivalent to heavy chronic smoking, and impossible to achieve the high levels associated with the first few drags on a cigarette. Nicotine does have effects on the body. It can contract blood vessels and increase the heart rate, hence the risks of high blood pressure, heart attack and heart rhythm disturbances if you smoke when you are taking NRT. Even if you don't smoke, you shouldn't overdo it with NRT.
There are a few circumstances when nicotine replacement could be harmful. If you have just had a heart attack or have a life threatening cardiac arrhythmia, NRT is not recommended. There is also a concern about NRT in pregnancy. It is hard to imagine anything worse for a developing fetus than tobacco smoke with its carbon monoxide and noxious chemicals. It is certainly harmful. Women who smoke throughout pregnancy run a higher risk of having a low birth weight or premature baby. The baby is also at higher risk for Sudden Infant Death Syndrome (SIDS). If, even with this information, a woman is having great difficulty quitting, I personally would have little hesitation about using NRT to help her quit.If you have just had a heart attack or have a life threatening cardiac arrhythmia, NRT is not recommended.
Bupropion - Zyban® - Prescription Drug
Bupropion is a tried and true antidepressant, known as Wellbutrin®. Zyban® is a 150 mg slow-release formulation of bupropion, specifically intended for smoking cessation. Antidepressants act on brain chemicals called neurotransmitters. Bupropion acts on neurotransmitters involved in the pathways for addiction and withdrawal from nicotine. The net effect is that someone taking Zyban® feels less like smoking and has less trouble with withdrawal. Zyban® is not NRT. You do not quit smoking on the day you start Zyban®. You actually take Zyban® for a short time, 7-14 days, and then quit smoking. If you start one of the forms of NRT on your quit date, you will have a better chance of quitting. You don't have to be depressed to try Zyban®. You just have to be a smoker. If mild depression (often sad or down, lack of energy) has been a problem for you, Zyban® may be a big help in quitting.
The standard recommendation is to start with one Zyban® a day for three days, then add a second dose eight or more hours later. The main side effects of Zyban® are dry mouth, tremor (shakiness) and insomnia (difficulty sleeping). As the TV commercials warn, you should not take Zyban® if you have a seizure disorder or a risk of seizure. This includes known seizure patients on medication, those people with a history of head injury and people who drink three or more alcoholic beverages a day. People who have an eating disorder, anorexia nervosa or bulimia, were noted to have a higher risk or seizures when placed on bupropion, and, therefore, should not take Zyban®.
Some notes about the side effects of Zyban®: If you are small and skinny, you may need only one pill a day. If you have problems with insomnia, take the second dose earlier in the day. Be sure the second dose is at least eight hours after the first dose. The risk of seizure is related to dose. The formula of Zyban® is meant to last eight hours. If you take your second dose less than eight hours after the first dose, you run the risk of having too high a blood level. Zyban® is Wellbutrin® is bupropion. If you are taking Wellbutrin®, you cannot add Zyban®. You are already on it!!
Quitting Smoking and Chronic Medication
When you quit smoking, your metabolism changes. Your body may eliminate some drugs faster and some drugs slower than it did when you were smoking. Your medication may have a weaker or stronger effect. Review with your doctor all the drugs you are taking on an ongoing basis and be particularly sensitive to any changes in their effects when you quit smoking. The doses may need to be adjusted.
Keep In Mind:
- It may take several tries before you succeed in quitting. Prepare yourself and look at each quit as a learning experience. Quit again as fast as you can. You have a better chance of succeeding.
- Every smoker is unique and needs different solutions. Examine your own habit closely and put together your own program.
- There are many techniques and medications to help you. You have the information. Pick out what appeals to you and try it.
- Millions of women and men have quit smoking. You can too!!




